 BU Visiting Faculty Dr. Emma Pitchforth (Senior Lecturer in Primary Care, University of Exeter) spoke this week at International insights: What can the development of community hospitals in international contexts tell us about their role in healthcare futures?, the first of three UK Community Hospital online seminars. Emma presented our NIHR study on Community Hospitals [1-3].
BU Visiting Faculty Dr. Emma Pitchforth (Senior Lecturer in Primary Care, University of Exeter) spoke this week at International insights: What can the development of community hospitals in international contexts tell us about their role in healthcare futures?, the first of three UK Community Hospital online seminars. Emma presented our NIHR study on Community Hospitals [1-3].
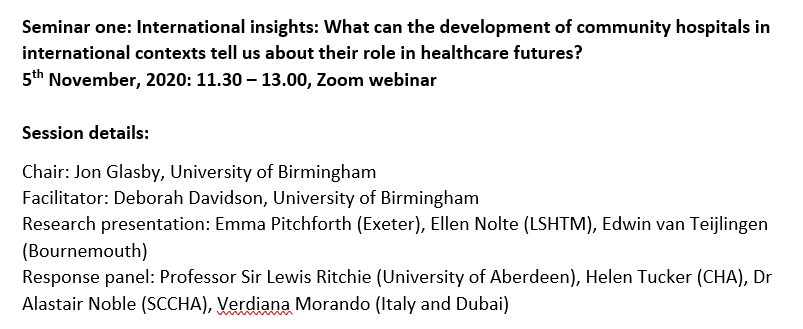 Community hospitals are a crucial but often neglected part of the health care systems in the UK. Community Hospitals are often very popular with local communities but they often face political challenges. COVID-19 has prompted us to make dramatic changes to way we think about and organise health care. Community hospitals have made a significant contribution to the health and wellbeing during the pandemic. The flexibility, resilience and strong community engagement typical of many community hospitals is being brought to the fore. At this critical time, questions are being asked about the future role of community hospitals and what lessons we can learn from other countries.
Community hospitals are a crucial but often neglected part of the health care systems in the UK. Community Hospitals are often very popular with local communities but they often face political challenges. COVID-19 has prompted us to make dramatic changes to way we think about and organise health care. Community hospitals have made a significant contribution to the health and wellbeing during the pandemic. The flexibility, resilience and strong community engagement typical of many community hospitals is being brought to the fore. At this critical time, questions are being asked about the future role of community hospitals and what lessons we can learn from other countries.
 The notion of a Community Hospital in the UK is evolving from the traditional model of a local hospital staffed by general practitioners and nurses and serving mainly rural populations. Along with the diversification of models, there is a renewed policy interest in community hospitals and their potential to deliver integrated care. However, there is a need to better understand the role of different models of community hospitals within the wider health economy and an opportunity to learn from experiences of other countries to inform this potential.
The notion of a Community Hospital in the UK is evolving from the traditional model of a local hospital staffed by general practitioners and nurses and serving mainly rural populations. Along with the diversification of models, there is a renewed policy interest in community hospitals and their potential to deliver integrated care. However, there is a need to better understand the role of different models of community hospitals within the wider health economy and an opportunity to learn from experiences of other countries to inform this potential.
There will be two further webinars at lunch time on the 12th and 19th November. You can register using the following link: https://bham-ac-uk.zoom.us/webinar/register/WN_dX8LwdHxQX2-Mf8nlt8nwg .
Prof. Edwin van Teijlingen
Centre for Midwifery, Maternal & Perinatal Health
References:
- Pitchforth, E., van Teijlingen, E., Nolte, E. (2017) Community hospitals: a traditional solution to help today’s NHS? Health Services Journal (11 July) https://www.hsj.co.uk/community-services/community-hospitals-a-traditional-solution-to-help-todays-nhs/7020019.article#/scientific-summary
- Pitchforth, E., Nolte, E., Corbett, J., Miani., C, Winpenny., E, van Teijlingen, E., Elmore, N,, King, S,, Ball, S,, Miler, J,, Ling, T. (2017) Community hospitals and their services in the NHS: identifying transferable learning from international developments – scoping review, systematic review, country reports and case studies Health Services & Delivery Research 5(19): 1-248.
- Wimpenny, E.M., Corbett, J., Miami, C., King, S., Pitchforth, E., Ling, T., van Teijlingen, E. Nolte, E. (2016) Community hospitals in selected high income countries: a scoping review of approaches and models. International Journal of Integrated Care 16(4): 13 http://dx.doi.org/10.5334/ijic.2463

 Our
Our 











 3C Online Social: Thursday 26 March 1–2pm – Research Culture, Community & Can you Guess Who?
3C Online Social: Thursday 26 March 1–2pm – Research Culture, Community & Can you Guess Who? INRC book roundtable/presentation by Drs Jonathan Cole and Catherine Talbot, Wednesday 22/04/2026, 13:00h, P426
INRC book roundtable/presentation by Drs Jonathan Cole and Catherine Talbot, Wednesday 22/04/2026, 13:00h, P426 BU M.Res. student’s evidence to UK Parliamentary Women & Equalities Committee
BU M.Res. student’s evidence to UK Parliamentary Women & Equalities Committee ECR Funding Open Call: Research Culture & Community Grant – Apply now
ECR Funding Open Call: Research Culture & Community Grant – Apply now ECR Funding Open Call: Research Culture & Community Grant – Application Deadline Friday 12 December
ECR Funding Open Call: Research Culture & Community Grant – Application Deadline Friday 12 December MSCA Postdoctoral Fellowships 2025 Call
MSCA Postdoctoral Fellowships 2025 Call ERC Advanced Grant 2025 Webinar
ERC Advanced Grant 2025 Webinar Update on UKRO services
Update on UKRO services European research project exploring use of ‘virtual twins’ to better manage metabolic associated fatty liver disease
European research project exploring use of ‘virtual twins’ to better manage metabolic associated fatty liver disease