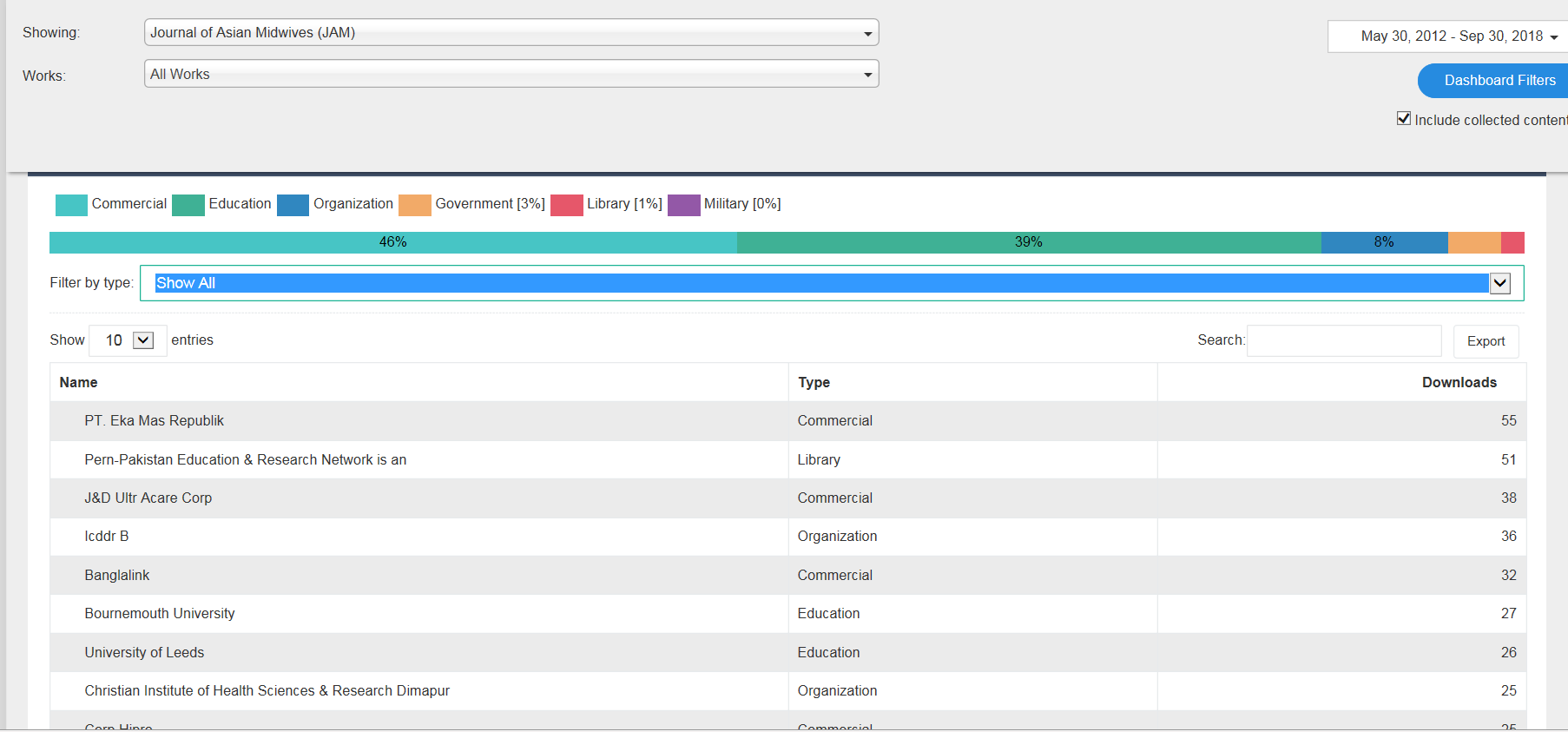
Congratulations to Lesley Milne, senior lecturer in midwifery, on the acceptance of her latest paper on maternity care in Nepal. This new paper ‘Gender inequali ties and childbearing: A qualitative study of two maternity units in Nepal’ will appear soon in the Open Access publication: Journal of Asian Midwives [1]. This is the second publication from a qualitative research study undertaken in two birthing facilities in Kathmandu Valley to examine barriers to women accessing these services from the perspective of hospital staff [2].
ties and childbearing: A qualitative study of two maternity units in Nepal’ will appear soon in the Open Access publication: Journal of Asian Midwives [1]. This is the second publication from a qualitative research study undertaken in two birthing facilities in Kathmandu Valley to examine barriers to women accessing these services from the perspective of hospital staff [2].
The study received financial support from Wellbeing of Women and the RCM (Royal College of Midwives) as Lesley won their first International Fellowship Award. The study was a collaboration led by Lesley in the Centre for Midwifery, Maternal & Perinatal Health (CMMPH) with two of FHSS’s Visiting Faculty, namely Prof. Padam Simkhada who is based at Liverpool John Moores University and Jillian Ireland, Professional Midwifery Advocate based at Poole NHS Hospitals Foundation Trust.

Well done!
Profs. Vanora Hundley & Edwin van Teijlingen
References
- Milne, L., Ireland, J., van Teijlingen, E., Hundley, V., Simkhada, P.P. (2018) Gender inequalities and childbearing: A qualitative study of two maternity units in Nepal, Journal of Asian Midwives (accepted).
- Milne, L., van Teijlingen, E., Hundley, V., Simkhada, P., Ireland, J. (2015) Staff perspectives of barriers to women accessing birthing services in Nepal: A qualitative study BMC Pregnancy & Childbirth 15:142 www.biomedcentral.com/1471-2393/15/142 .



















 Dr. Paul Whittington attends Technology and the SEND Reforms Roundtable in the House of Commons
Dr. Paul Whittington attends Technology and the SEND Reforms Roundtable in the House of Commons Dr. Paul Whittington joins Bett 2026 DfE Assistive Technology Roundtable
Dr. Paul Whittington joins Bett 2026 DfE Assistive Technology Roundtable BU Prof Jonathan Parker promoting social work in Malaysia
BU Prof Jonathan Parker promoting social work in Malaysia New interdisciplinary paper accepted for publication
New interdisciplinary paper accepted for publication Horizon Europe Cluster 3 (Civil Security for Society) 2026 Calls Now Open
Horizon Europe Cluster 3 (Civil Security for Society) 2026 Calls Now Open MSCA Doctoral Networks 2026 Call Information Webinar
MSCA Doctoral Networks 2026 Call Information Webinar Reminder: Register for the ESRC Festival of Social Science 2026 Information Session
Reminder: Register for the ESRC Festival of Social Science 2026 Information Session ECR Funding Open Call: Research Culture & Community Grant – Apply now
ECR Funding Open Call: Research Culture & Community Grant – Apply now ERC Advanced Grant 2025 Webinar
ERC Advanced Grant 2025 Webinar Update on UKRO services
Update on UKRO services European research project exploring use of ‘virtual twins’ to better manage metabolic associated fatty liver disease
European research project exploring use of ‘virtual twins’ to better manage metabolic associated fatty liver disease